A doctor shouldn't need an informatician to ask a question. AI data agents are changing that
For the first time, domain experts can query their own data in plain language, no engineer in the middle. I built a genomic data agent on Microsoft Fabric and Copilot Studio that clinicians use right inside Teams.

🩺 A doctor shouldn’t need an informatician to ask a question. AI data agents are changing that.
Everyone talks about ChatGPT or Claude writing emails or generating code. But the shift I find most profound is quieter and more fundamental: for the first time, domain experts can talk directly to their data - without an engineer in the middle.
Let me explain what I mean.
🎙️ LLMs as universal translators
When LLMs became mainstream, what made them revolutionary wasn’t just that they could answer questions. It was that they lowered the barrier to an entire world of machine learning and data systems that previously required years of technical training to access.
Think of an LLM as an assistant that speaks almost every language simultaneously: Python, SQL, R, Bash, and yes, even genomic languages like VCF or FASTA. The LLM doesn’t just understand your question. It can translate it. From natural language into a database query, an API call, a script.
That translation layer is what changes everything.
🧬 The problem it solves - a real example from genomics
Imagine you are a clinician. You have a patient with an unusual combination of symptoms and you suspect a rare genomic variant might be the cause. You want to know: has anyone seen this before? Is there a patient in our historical data with similar symptoms and a matching variant?
To answer that question, you have to ask a bioinformatician or data analyst. They write SQL queries against internal databases, maybe chain together some Bash scripts, pull results from multiple sources, and come back to you - sometimes days later - with an answer.
And that is actually the optimistic version of the story. Because sometimes there is no clean database at all. Sometimes the data lives in a network share nobody has touched since 2019, buried inside Excel files named “patientXY_final_v3.xlsx”. Each one lovingly maintained by a different person, in a slightly different format. Your bioinformatician is not writing a query. They are on an archaeological dig.
And then you have a follow-up question. Maybe about allele frequency. Maybe about the clinical presentation of that historical patient. Back to the queue.
This chain of communication is essentially the telephone game. Context gets lost at every handoff. The analyst interprets the question, the doctor interprets the answer, and somewhere in between the nuance disappears. It is slow, it is lossy, and critically - it keeps the domain expert away from their own data.
🚀 What is now possible
To make this concrete, I built a prototype of exactly this: a genomic data agent that a clinician can query in plain language, directly in Microsoft Teams or Slack, from any device.
And guess what - building it was even more fun than writing the queries and providing the answers myself. I am pretty confident other informaticians will feel the same. 🙂
The architecture underneath is a data lakehouse built on Microsoft Fabric, pulling from three sources: the 1000 Genomes Project , ClinVar, and the Human Phenotype Ontology (HPO). These are layered along a medallion architecture - raw data, curated data, and a semantic model on top. Using Fabric’s native AI capabilities, semantic models, and few-shot prompt engineering, I instructed a data agent to understand genomic queries in natural language and translate them into the right queries across that data.
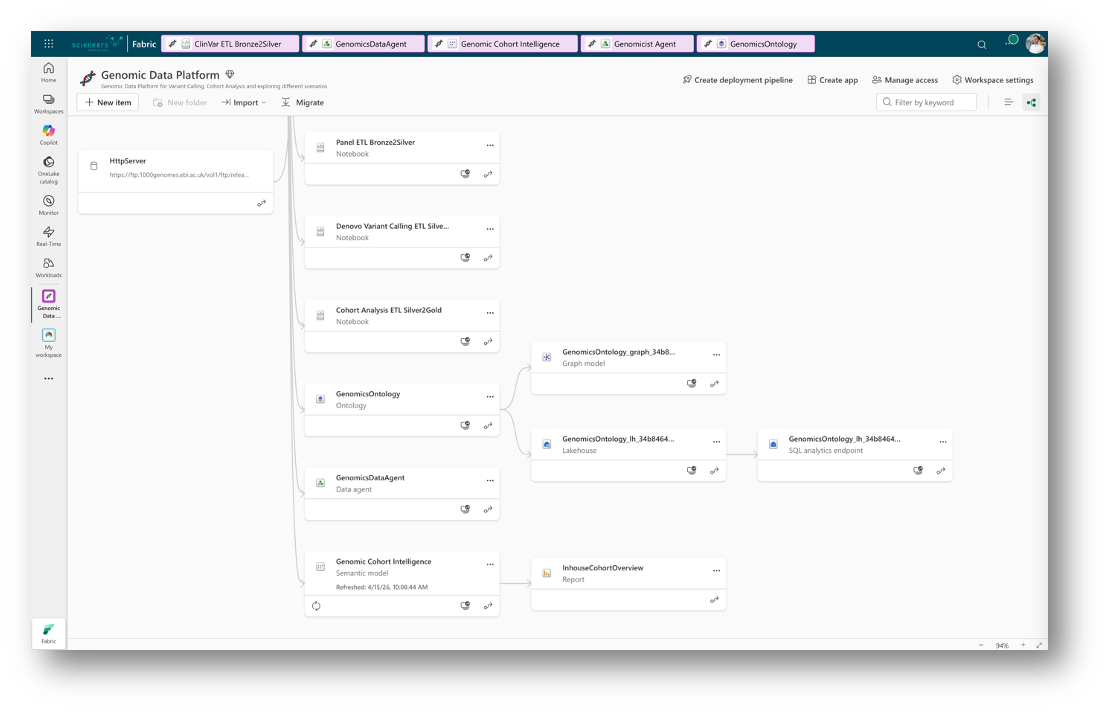
The Fabric canvas - from raw ingestion to semantic model and data agent
The agent was then deployed through Copilot Studio and shared directly in Teams: Accessible to anyone in the organisation, no SQL knowledge required.
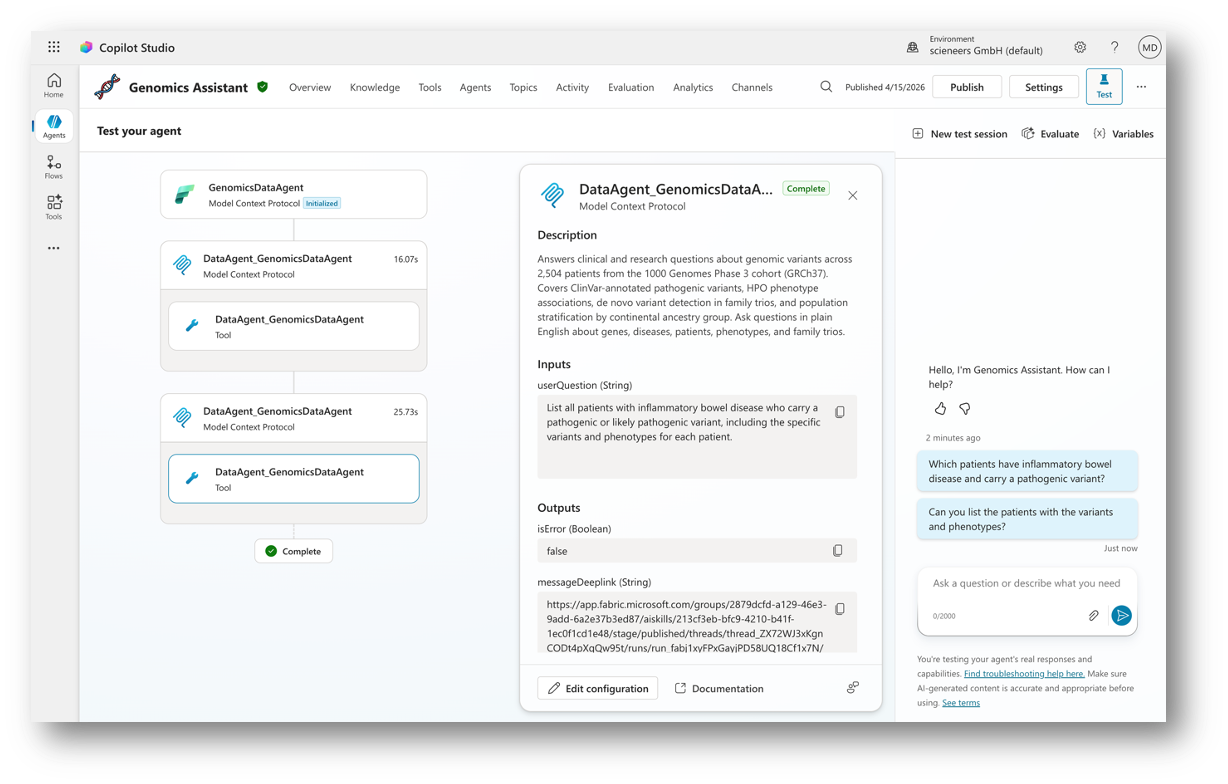
Agent configuration and live testing in Microsoft Copilot Studio
In the demo you can see it in action. A question you would have previously waited hours or days to get answered comes back in seconds. The latency of the AI itself, not the latency of a broken process.
A Genomic Data Agent in Microsoft Teams - Live Demo
A few notes on the demo: the HPO phenotype assignments are randomly generated for demonstration purposes. The underlying genomic data is sourced from the 1000 Genomes Project, which reflects genomic data from mostly healthy individuals not clinical patient records. The video has been cut for brevity. Actual response latency is between 5 and 20 seconds depending on query complexity.
🏗️ But the agent is only half the story
It is important to be clear about something: the data agent alone is nothing without a solid data platform underneath it.
In this demo I used Microsoft Fabric and a lakehouse architecture but the same principle works with Data Lakehouses build in Databricks, a classic relational database, a NoSQL store, or even a graph database. The right choice depends on your data, your domain, and your organisation. What matters is that the data is somehow structured, curated, and queryable. The LLM handles the translation. Your data platform handles the truth.
And this is precisely where LLMs become so compelling as an interface layer: they speak all of it. SQL, Spark, Cypher for graph databases, document queries - it does not matter what sits underneath. The domain expert asking the question does not need to know. They just ask.
🚧 So what is holding us back?
In medicine, the honest answer is regulation, mostly for good reason. Clinical data is sensitive, identifiable, and governed by frameworks like GDPR and national healthcare laws that often restrict where data can live and who can query it, especially in Germany. Building a data agent on top of real patient records is not simply a technical problem. It is a legal, ethical, and organizational one. That friction is not going away, nor should it entirely. But in my opinion we have to find a way to utilize this technology within those boundaries, because done right, it will bring direct and measurable benefits for healthcare and patient outcomes.
But outside of medicine, in industries where those constraints are looser, the barriers are much lower. The technology is ready. The data platforms exist. The agent layer is mature enough to deploy today.
The question for many organizations is no longer “can we do this” - it is “do we have the data culture, the architecture, and the will to make it happen.”
💬 What is your view?
Are regulatory constraints the main blocker in your domain, or is it something else like data quality, organizational silos, trust in AI outputs? I work in this space and regulation is still the wall. What is your experience?
Happy to go deeper on the technical architecture: Fabric setup, data lakehouse concepts, the few-shot prompting or (data) agents in general. If there is interest drop a comment or reach out directly.